Let me introduce Dr. Anne Robert's. Dr. Ann Roberts and Empire Medical Training has been working together with her for many years - at least 15 years or so. She has a very busy practice in Springfield, MO and she is board certified internal medicine physician, multi-specialty trainer and in aesthetics. She is a graduate of Yale medical school and her undergrad at Johns Hopkins. Anne did her residency at Mayo Clinic in Rochester, MN and Scottsdale, AZ.
Thank you so much Steve for introducing me and yes, I'm working with empire for a number of years and yes, I did my formal background training in internal medicine at Yale University and Mayo Clinic.
Over the years, I have kept my boards in internal medicine but along the way I did some research and actually it was in stress and I found was stress hormones, which cause calorie burning, that men respond more vigorously with their calorie burning than women. That started my interest in these fields and now able to integrate a testosterone and bio identical hormones and some integrative functional medicine into my internal medicine type practice.
That's what I wanted to be able to share with you and Empire asked me to go over about testosterone therapies and this is an exciting thing to be able to do for your patients. If you look at the market share this area in BHRT is certainly growing. The incidents of testosterone deficiency are rising in America, and certainly all aspects of bioidentical hormone replacement and will keep increasing as the baby boomer demographic ages that many of us might actually be in. Patients want to maintain their function, their health, and their quality of life as they get past midlife. The growing awareness of what this could do for patients as well as the growing skillset in physicians is going to lead the way in this field which is expected to grow exponentially.
You can see that here on this bar graph which is showing you in different colors the growth of the different types of hormone replacement therapy. The female estrogen or progesterone or progesterone type of hormone therapy still has the biggest market share but you can certainly see that the other types of hormone replacement certainly have grown, including testosterone.
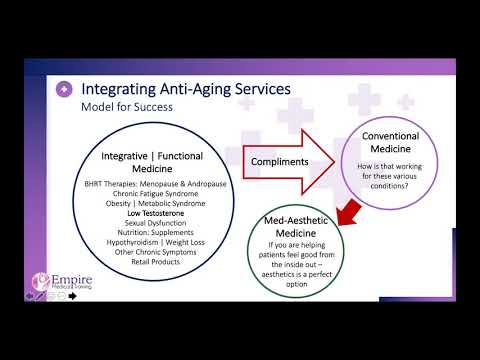
This is what empire asked me to talk a little bit about today and I've lectured for them for their different classes about bioidentical hormones for a number of years. This is something that I'm quite comfortable with and we're going to be giving you a little overview today and looking at integrating these Anti-Aging services into an overall practice.
What patients are starting to look for from a medical practice today is that their physician can integrate both the rich skillset in a traditional manner, pharmacy management, all the traditional medical procedures that all of us do in our practice with bioidentical hormone replacement.
Some of you may desire to work with nutrition and certainly Empire trains in all aspects of functional medicine. These are things that patients really would like their regular physician to be able to manage both the traditional medical model as well as functional medicine.
There are many ways to integrate testosterone therapies or a skillset that you should have if you would like to do this. Many of the different types of conditions that hormones administered in an correct and customized way can really help patients with many, many different medical conditions.
You see a list of those on the left, and that's everything from weight management to menopause to today's topic of testosterone replacement in males. You can really make a huge difference in a patient's quality of life and at the same time probably really do a better job as far as managing their health while growing your practice - this is what patients really are looking for.
This slide is showing on the right an age-related decline in testosterone levels and certainly this is going to be associated with many different things. When you key in on levels normal as you age, what are some of the benefits? Number one, you look at the top bone mass and we know that testosterone and all androgens are actually anabolic. This means they promote tissue integrity and certainly we know that they help with bone mass so we will lose less bone as we age our hormone levels.
Testosterone is the hormone of all the different bio-identical steroid hormones that needs to be in the narrowest range of safety. Not too high, but also not too low and when we optimize that we can help with many parameters such as tissue integrity and many of the different connective tissues.
Testosterone at normal levels can help with things like optimizing blood sugar again not too low, but also not too high. Here are some metabolic consequences of having abnormal hormone levels. Certainly, the third bullet point down, sexual function, is what many patients are going to come in talking to you about but you need to understand what you're working with.
That's what I want to give you a little overview of today, is how to think about working with this so you can decide if testosterone replacement therapies is something you'd like to add to your practice. Certainly, if patients are testosterone deficient and you optimize their testosterone levels it does help sexual function for both genders.
Actually though, today we're focusing a little bit more on male testosterone replacement. Anabolic substances such as testosterone or all androgens will help with body composition, muscle to fat ratio, and muscle which is certainly associated with survival and many chronic diseases and longevity - it's certainly associated with metabolic health.
Remember, muscle is where our mitochondria are concentrated and burns our calories so indirectly helps a lot with weight management and some muscle to fat ratio as well as improved abdominal obesity. Again, only keep testosterone levels in its narrow, normal range which is important for body composition.
We know that in the brain testosterone is an agonist of dopamine, norepinephrine, and serotonin. All three of these are associated with good mood specifically associated with serotonin and dopamine, and the stress hormone - catacholamines like epinephrine - norepinephrine.
That's more of an indirect effect and that was something my research actually was looking at many years ago. Specifically, serotonin and dopamine, which we all know helps with mood. Certainly, many people feel like if you look at that second bullet point for the bottom, while this is not going to cure things like Alzheimer's or other neurodegenerative disorders.
Testosterone probably has some neuroprotective effects when all of our hormones are balanced appropriately. Many people actually think there's a growing thought that some of the age-related normal decline in cognition as we age is associated with less dopaminergic activity in the brain.
Testosterone being a dopamine agonist probably helps a little bit with that and all the hormones being balanced together that will optimize and perhaps become somewhat neuroprotective against neurodegenerative disorders.
This slide is looking at some of the things we'd want to consider as we're thinking about testosterone therapy and these are the things that are going to be so important for you with some of your medical patients. Let's look on the left first, what are some of the benefits? Certainly, sexual dysfunction - no question, this is absolutely going to be helpful for patients that are having EDD. I will specify overdosing will not help sexual dysfunction if patients are normal to begin with but will work certainly in a proper range. We know many men, midlife and beyond, have a testosterone deficiency and extremely helpful for bone density - it's anabolic. This is true for both genders, sexual function and mood.
First of all, when we have optimal hormonal levels all the different hormone levels that are optimized and in proper balance optimizes many things like our glucose levels and insulin sensitivity, et cetera. As hormones and glucose levels become out of balance we move toward metabolic syndrome, physiology, insulin resistance, which is associated with obesity.
That is a metabolic way that adequate normal testosterone levels can help. Number two is body composition and muscle to fat ratio. When we have enough of anabolic substances like testosterone it helps us maintain a good body composition of good muscle to fat ratio as we age. That's very important because muscle is where mitochondria is concentrated and certainly helps burn our calories.
Third, and this is relevant to the research I did years ago. we know that stress hormones, like epinephrine and norepinephrine are a major pathway by which our metabolic rate or the calories we burn by just sitting still like all of us are now.
Our metabolic rate is mediated and moderated, we have known for a long time that stress hormones like epinephrine and norepinephrine raise our metabolic rate and this is so that we can have our fight or flight response in case we are in a life or death situation which allows us to survive that.
That's how we developed revolt and what I looked at years ago was whether men or women had differences in their metabolic rate or their calorie burning response. With just the stress hormones, I found that men had a greater response from the calorie burning aspect and metabolic cardiovascular response.
Since that time, it has been documented that testosterone sensitizes neurotic receptors that are stimulated by epinephrine and norepinephrine. We know that these receptors are a major moderator or mediator of the calories that we burn just sitting still like we all are right now. If we burn more calories for an hour just sitting still then our weight is much more likely to be able to maintain being maintained at a normal level.
That particular effect is interesting, if you took two identical twins one is testosterone deficient and say they go out and exercise vigorously which releases stress hormones, the one with normal or adequate testosterone will burn more calories during that intense exercise because than the other since his response to that stress hormone release is going to be sensitized by having enough testosterone. These are the three ways that testosterone can affect your weight and muscle mass.
I mentioned the glycemic control and some sensitivity. I mentioned quality of life, memory, and cognition which you hear that a lot from patients. In addition, patients mention just that spark in personality, assertiveness, and getting excited about things in life - that's largely a dopamine effect. We all know serotonin is a little bit more of a Zen neurotransmitter like happiness, contentedness, and things like that and dopamine we often call the power neurotransmitter - these are things testosterone can do for your patients.
Now on the right, these are also very important. What are some things that we need to consider for not receiving testosterone treatments? Anybody with an active prostate cancer or an active hormonal cancer which any sore breasts would be included but that is not an exhaustive list with those two largely going to be a contraindication.
People that have been adequately treated for prostate cancer and there are some studies when their testosterone deficient now coming out about it as not being unsafe. In reality, as all of you that are probably primary care type practitioners are concerned about harm to your patient or danger have an oncologist clear that patient. If an oncologist has cleared that patient and they've been treated in the past and they've cleared them for hormones then you do this in a sensible, safe manner and you monitor levels. Then that's something that could be certainly a safety mechanism for yourself is to have an oncologist clear that patients - we do not clear those patients.
Second bullet point down on the right, we do not recommend oral testosterone. I don't use sublingual either because about 30% to 40% of that is swallowed in the saliva but we do know oral is really toxic to the liver. We just have better delivery forms that we can use now and certainly anybody with BP H we have to be cautious to stress to will usually increase the size of the prostate in that situation may cause urinary retention or necessitate a procedure.
This is something that is a soft contraindication, sleep apnea as well and sometimes it is used but you really need to watch those patients closely clinically. If you can get where you need to go in those patients without starting testosterone or all start at a very tiny starting dose - that's probably safer for those patients.
The fifth bullet point down is diastolic dysfunction or the stiffening of those ventricles and they of course come up with different names, and acronyms every so often but it's really the stiffening of the ventricles that we're talking about because the hardest muscle.
Testosterone is anabolic and improves muscle strength and contractility and so that's really what it's talking about. Not so much systolic, but more diastolic, but you do need to watch that very closely and really being in consultation with a cardiologist in terms of heart as well. We do know that Testosterone does slightly increase clotting factors and is going to cause a relative cytosis and so there'll be some slides talking about certainly watching those things, monitoring a CBC for instance. There are not good recommendations right now for monitoring the coagulability. I always balance the testosterone with something simple, like a baby aspirin or fish oil - something like that.
When you have a patient say that he has stints in their heart and things like that it's probably a great idea to just be in consultation with a cardiologist about that as well so that you make sure testosterone is a safe thing for you to be doing for them.
I always try to be proactive to balance patients with a little bit of fish oil, baby aspirin or whatever you think is appropriate. You are going to want to certainly monitor the level and you're going to want to monitor the hemoglobin hematocrit for the relative erythrocytosis.
Liver function is usually fine unless you use the oral or sublingual lipids and then of course we all know that testosterone can cause a little bit of oily skin and occasionally acne. If you have some patients that are acne prone, you just want to start at a more conservative starting dose.
If your patients are heavy and obese some of our testosterone in all individuals is going to be converted into estrogen. The heavier we are, and certainly as Americans we're heavier than we probably should be, Testosterone may be converted over to estrodiol, and that's by an enzyme called aromatase and it's most active in that. Then if that happens excessively you might get a little bit of breast tenderness so we always like to monitor the estrogen levels as well as the testosterone. So those are a few things you want to kind of think about as you're deciding whether you'd like to start your patients on testosterone therapy or not.
I do want to mention to keep those testosterone levels in that normal range because we have data, we don't have data that that's going to increase the risk of prostate cancer. I think that's an important thing that you can look at to reassure yourself and just a review of some of the things that I mentioned. This is probably reasonable as urinary tract symptoms would be urinary retention. This is really a good review and a good safety list that Empire has provided to you.
These are some of the guidelines and I alluded to them already, measure patient’s PSA at three months after injections - you want to baseline it three months after starting. It should never more than double, and it should never ever go outside the reference range or they need a urology work up. If you have two in a row that are elevated, always recheck estrogens as well as testosterone. Certainly, most prostate cells do certainly have androgen receptors so while it may not have initiated a cancer it may cause something to grow.
This next slide is an overview of the different types of forms of testosterone, and we're going to cover each in a little bit more detail. Injections are how most of us were trained and you see the different forms at the bottom. You also see the different advantages at the top, pellets certainly are another type of mode of administration. Testosterone pellets have been around a long time and they are put in the fat subcutaneous fat tissue usually in the gluteal area, but there's some practitioners do put them in the lower abdomen. About the right dose, you're always going to want to check some levels as you're starting, You are going to have a more consistent level without big peaks and troughs like you might get sometimes with your injections. It's a short 5 minute procedure maybe 15 at the most under local anesthesia.
You do need to do it properly. Empire has a fantastic Hormone Pellet course where you go over the insertion procedures. The procedure is very easy but of course you could get bleeding, bruising, or possible infection. I generally do not use sublingual or tat or oral because of the liver toxicity but certainly some practitioners still use the sublingual.
Most physicians do not use oral testosterone anymore, certainly if you're going to use that sublingual, you'd want to be careful to avoid having him swallow that saliva. The problem with the patch is just so much contact dermatitis and as allergies to the patch so this is not quite as popular as it was at one point.
Then you have these other modalities that have come a little more popular - topicals are another very popular way to administer Testosterone. These can be the pharmaceutical, hydro, ALC, alcoholic gel, or can be compounded and then you have infinite dosing and control. The dosing is more for the AndroGels and you'd start at the lower level for those.
You would want to check Testosterone levels in four to six weeks after that. Generally for compounded Testosterone start anywhere from seven to 20 milligrams per day and the Anti-Aging course is a great course to go over details really of that topicals and avoiding household spread.
This is a table that showing you an overview and certainly I always advocate customizing your dose to the levels of your patients. This is extremely important that these are some common types of doses with considerations over there at the right to think about as you're using those.
In terms of levels, serum levels can be obtained, saliva levels, and urine levels. A finger stick is a blood spot level and certainly the Anti-Aging course goes into great detail about the differences of those that you see at the top for serum level and here are some of the recommendations from the endocrine society.
PSA levels is mandatory before, at three months, and at six months. I mentioned the parameters and guidelines earlier and as aforementioned only patients who are deficient really should be given testosterone.
Testosterone is a controlled substance so we want to be safe with this. We want to do this in a precise manner and tailor it to that patient's level and again consider cardiovascular concerns.
I work a lot with nutritional medicine and functional medicine. These are some nice adjuncts, and we talk about these more in the Hormone Pellet and the Anti-Aging class but that can either help raise testosterone and naturally help with prostate with the breakdown of our hormones. They're broken down in a healthier pathway so these are a lot of great recommendations that you may wish to consider using with your patients.
Now, as far as pricing and packaging which is highly geographically variable, how you're going to price yourself? These are some suggestions that Empire has and I think that you want to always put quality first - so I wanted to be sure and convey that to you. I firmly believe that testosterone therapies can grow your practice - no question. We want to first do a good job, but here are some of the different types of monthly strategies that physicians employ for charging patients which are becoming more and more popular out there.
You can see some of that at the bottom of the screen and that's something that some of you may wish to consider as a practice but do a great job. The top of the slide refers to if you were consulting with them for other health conditions as well or a medical examination and whatever else you're including in the package pricing.
Then some of you may wish to do saliva and some serum testing which is noted. You see that there are PSA tests included in the packages which we are all accustomed to doing. Some of you are working with insurance and some of you are not, so you'll need to think about that and how you would like to do that as you work with your patients.
Again, these are a summary of the last slide and some of the different pricing strategies and I will say, Empire has a great Pricing and Packaging document. I believe it's for members but I shouldn't speak out of turn but is a wonderful document and a way to know how to price yourself across the country because that is important.
For you to know how to price yourself, some practices if you do that monthly fee most are going to prescribe it since it's a controlled substance. The vial or whatever form of the compounded medicine is prescribed per patient, the pitfall is when the medicine will be sent to the patient which is picked up at the pharmacy by the patient.
Many patients already know how to self-administer intramuscular injections so that's really up to you and how you feel comfortable doing that. Whether you're using a long acting or short acting form for intramuscular testosterone, check with the patient whether that's amenable to them. These are a few things that you may wish to consider as far as your pricing - Empire has outstanding classes in these topics and adjuncts such as pellets.
This is a great course to help you if you want to master hormone pellets. Anti-Aging is where the physiology is covered in depth and is also a full one day class that's a really fun and popular class as well as sexual dysfunction.
These are all wonderful adjuncts - Questions and answers.
Do you dose the testosterone based of the total testosterone level or the free testosterone level, and what is the goal range for testosterone levels when using testosterone therapy?
It's not a super short answer but yes, I think that free is more accurate but what you saw on that slide that we had a few slides ago was total testosterone and those are the guidelines you see most in the literature. Free testosterone is not taking into account the binding proteins which are going to act like little sponges and suck up that testosterone floating around in the bloodstream so the free testosterone will always be more accurate.
Some of you may wish to test for this that are in more functional medicine or integrative type practices.
Should we do saliva or urine testing?
If you are using serum and we know that typically that's going to because of the binding protein effect, underestimate a little bit the amount of testosterone in that patient and so maybe you don't go right up to that hundredth percentile that your lab gives you as that reference range.
Always use your reference ranges no matter what lab you use, show that you kept levels in a normal level and always on the chart. If you're using saliva or urine you probably could make your goal a little bit higher. However, two things, only use what you need to alleviate the patient's symptomatology and you do not have to get right to that upper reference range or the 75th percentile or the 90th percentile - you don't have to. Number two, remember what side effects could occur such as male pattern hair loss that could happen. Oily skin or acne could happen, if the male patient gets up in the middle of the night three times and he tells you that maybe that prostate's getting a little bit too big and so you want to look for intervening side effects. Then depending on what level they are, you may want to stop at that 50th percentile and not go any higher because we always want to be safe with our patients.
How do we balance this therapy without shutting off the body's natural regulators as well as not overdosing to prevent unintended effects?
The truth of the matter is when we give hormone, we are going to be enacting that negative feedback loop where our body senses we've got enough testosterone out there and I don't need to make as much. This is another great reason to keep in a normal range and not overdose because we do know that with testosterone in males is going to go back up to the brain and relay back that we've got enough testosterone out here. You can stop making as much and so the FSH and LH those two Metairie substances are going to go down a little bit and therefore we won't make as many sperms - so the sperm count will go down with testosterone use typically.
Then we won't be synthesizing as much testosterone in the testes because the LH has gone down. So the testes that make testosterone aren't getting that stimulation to make as much and so you do tend to see a little bit of decrease in testicular volume, maybe 10 to 15% which is pretty typical.
If somebody wants to maintain male fertility and they have too much testicular volume loss. There are other things we can do in kind beyond the scope of this course that I always discuss in the Anti-Aging class where we go over the questions, certainly.
That be directed to empire, that's kind of longer subject, but there are things like hCG that can be used to stimulate the latent sperm cells and decrease the volume loss. So there are some solutions for that.
As far as the conversion into estrogen, there are some solutions for that too. Weight loss is the obvious first choice, but there are other things that sometimes we can use such as tiny doses of aromatase inhibitors or natural substances such as chrysin which can be used to decrease some of those other side effects.
Are you ready to reopen your practice and start generating new revenue?
Empire Medical Training is your source for valuable Procedure training and insight into learning new procedures and growing your practice.
Join us this Thursday May 14 at 2:00 PM EST with Dr Cosentino, president of Empire Medical Training and Anne Roberts, MD, Renowned Anti-Aging and Wellness Physician, with credentials from Yale School of Medicine and residency trained from Johns Hopkins University.
Bioidentical Hormone Therapy continues to surge in popularity and by offering Testosterone and many other hormone therapies to your practice, you can help meet the increasing patient demand while significantly growing a new revenue center in your outpatient, practice setting.
Empire Medical Training offers the most expansive curriculum and certification in Anti Aging medicine for the past 22 years. The training provides up to date and practical information you can immediately implement into your practice, to help you develop a thriving Anti Aging practice.
Here is what you will learn
Testosterone Therapy for Men
1. How do I implement Hormone Therapy in my practice?
2. Opportunities to adding Testosterone and Hormone therapy to my practice?
3. Benefits of adding Testosterone Therapy to my practice.
4. Method of Treatment relating to Testosterone therapy.
5. Types of Treatments.
6. Testosterone Dosing and Monitoring.
7. Recommendations and Guidelines.
8. Treatment Pearls.
9. Risks associated with Testosterone therapy.
10. Business Pearls for developing a Thriving Hormone Practice.